
![]() Click each graph to explore the data:
Click each graph to explore the data:
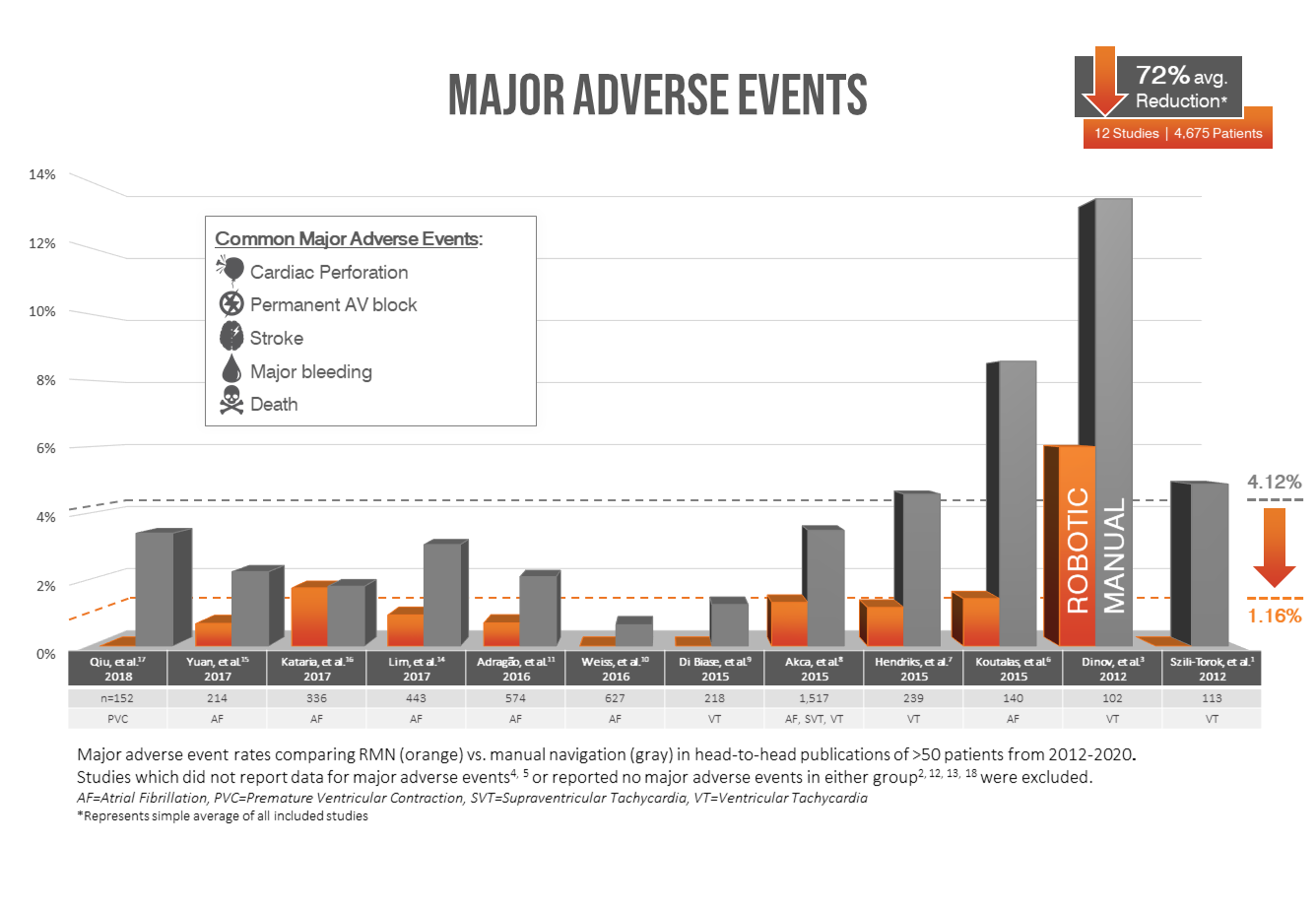
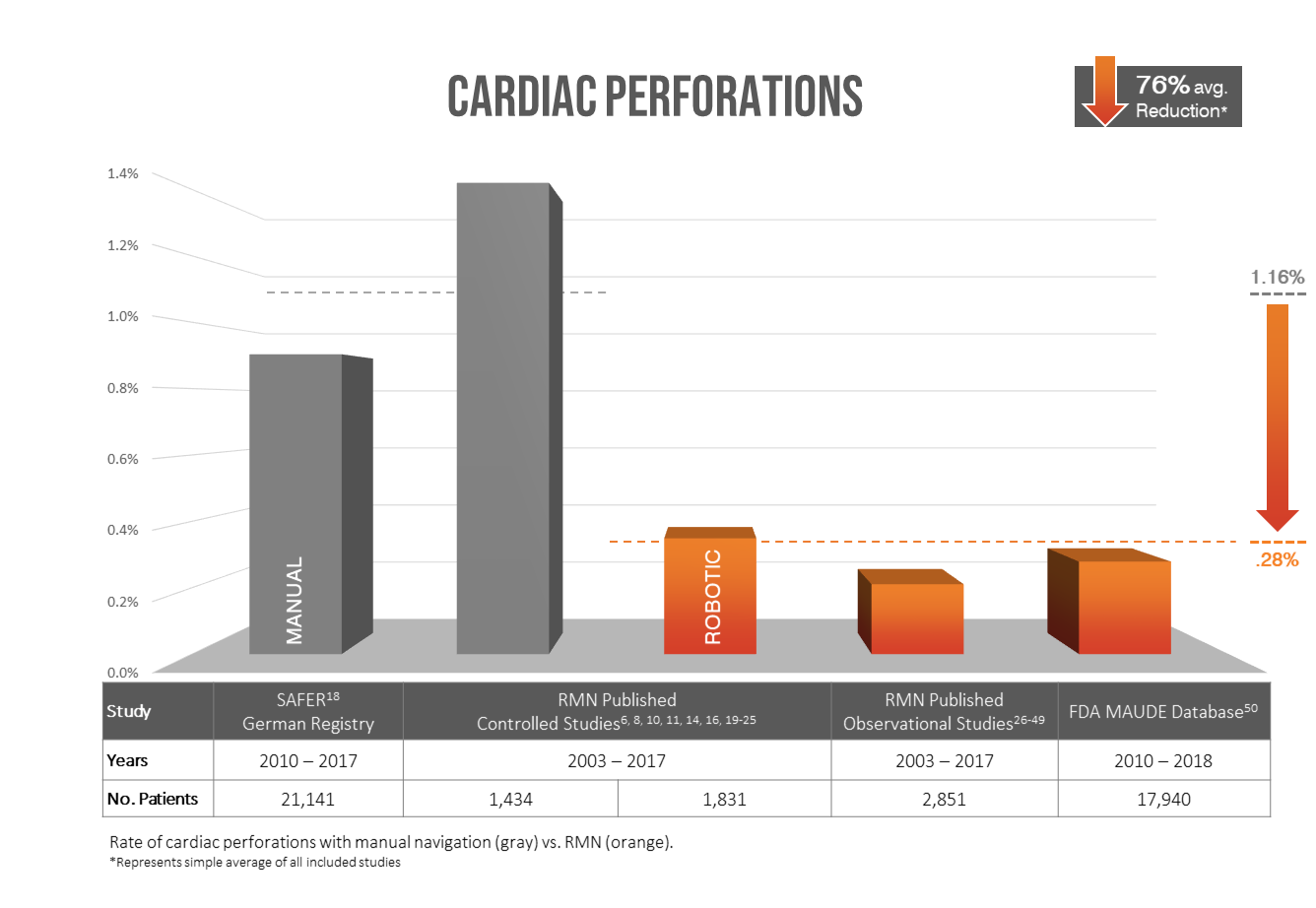
Clinical Validation
Data Transparency
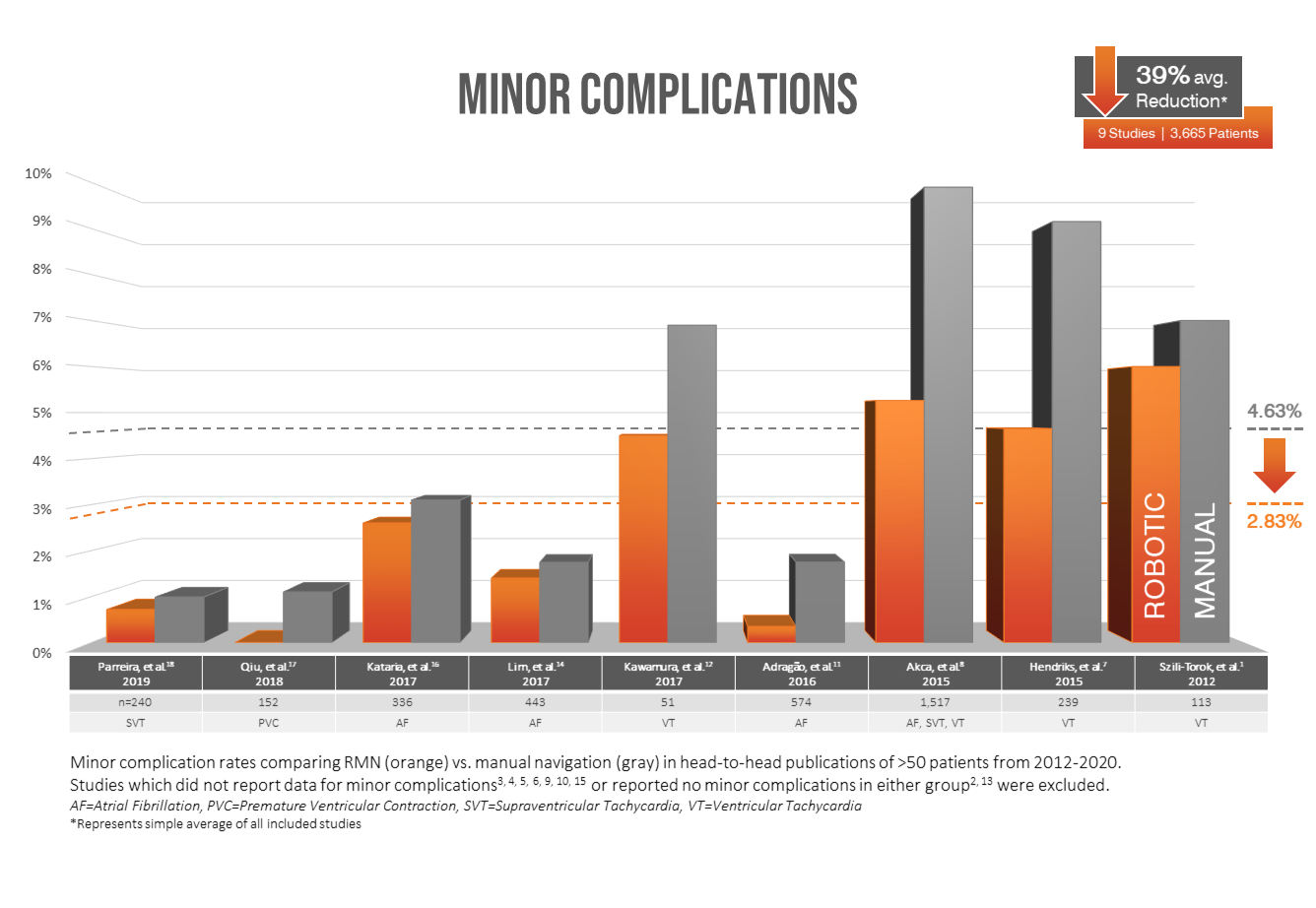
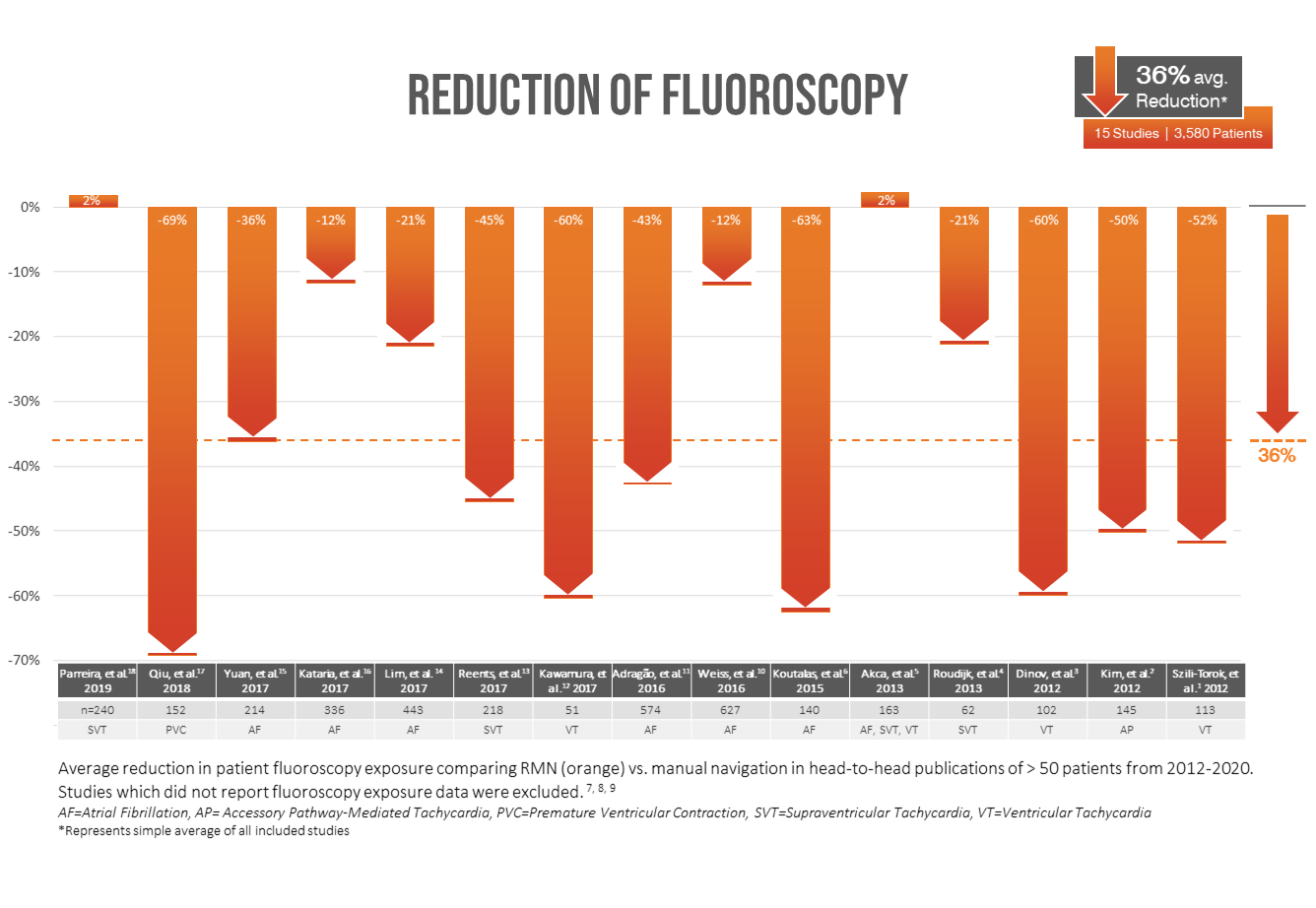
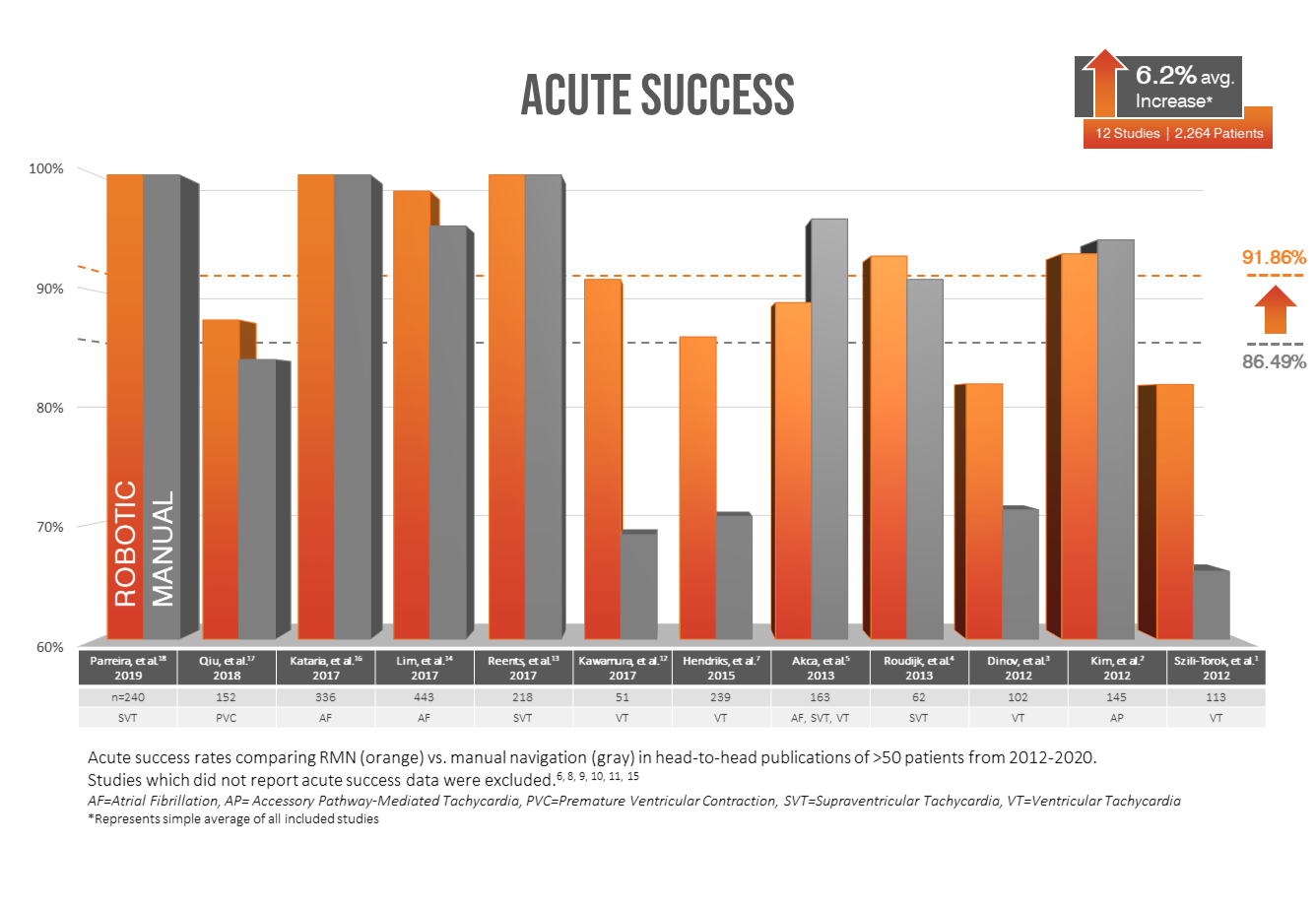
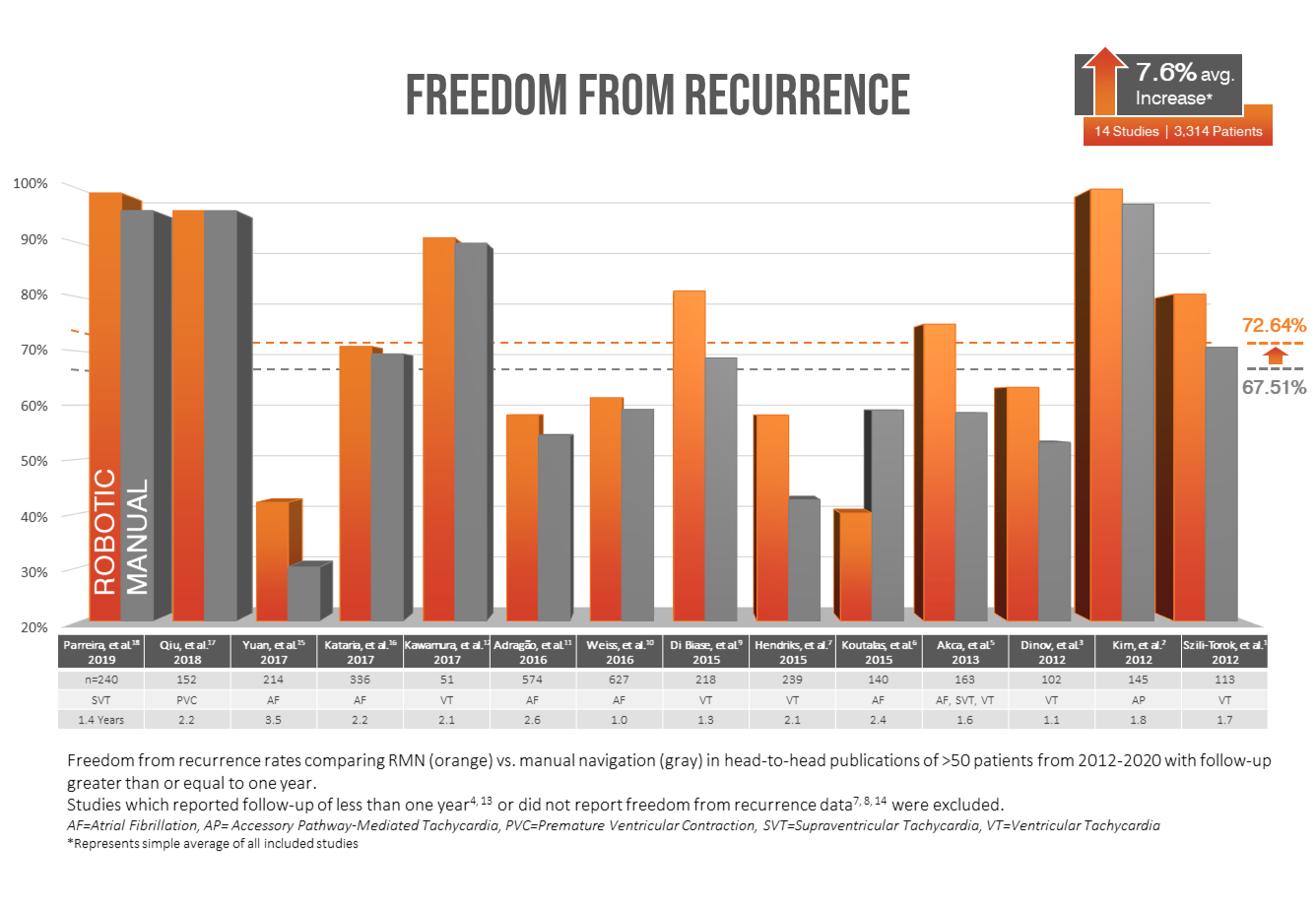
We believe data should be presented clearly and comprehensively. The data summarized here includes all known data from all known publications describing:
50+ Patients
Robotic vs Manual
2012 - 2020
Clinical Dossier
A Sample of Clinical Literature
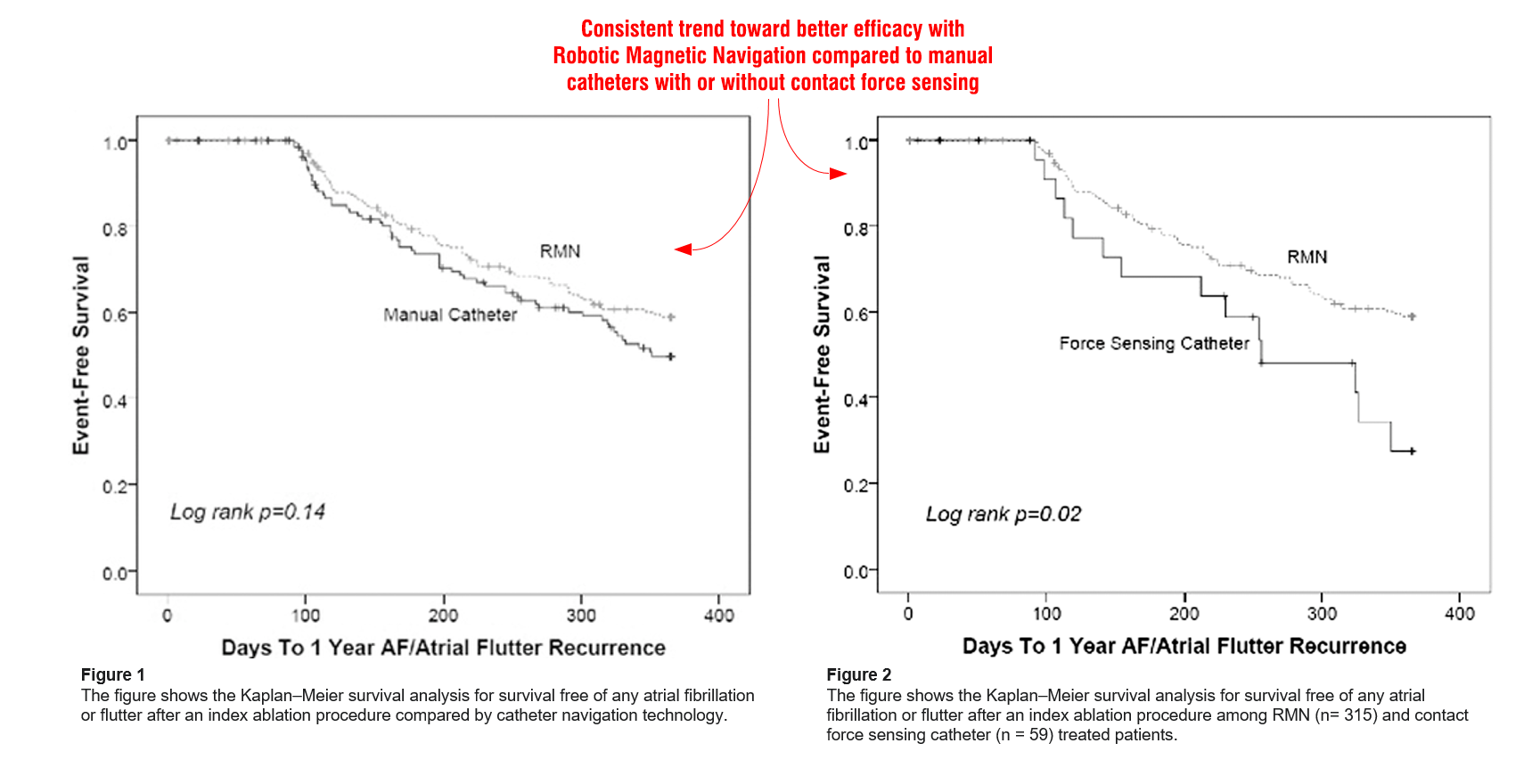
A Comparison of Remote Magnetic Irrigated Tip Ablation versus Manual Catheter Irrigated Tip Catheter Ablation With and Without Force Sensing Feedback
Weiss JP, May HT, Bair TL, Crandall BG, Cutler MJ, Day JD, Osborn JS, Mallender C, Bunch TJ | Journal of Cardiovascular Electrophysiology. Vol 27, Suppl 1, pp S5-S10, March 2016
BACKGROUND:
Remote magnetic navigation (RMN) and contact force (CF) sensing technologies have been utilized in an effort to improve safety and efficacy of catheter ablation. A comparative analysis of the relative short- and long-term outcomes of AF patients has not been performed. As such, we comparatively evaluated the safety and efficacy of these technologies.
METHODS:
A total of 627 patients who underwent catheter ablation with either a manual irrigated tip catheter: (312, 49.8%) or by RMN: (315, 50.2%) were included in this single-center cohort study. Patients treated with CF (59) were analyzed separately as well. One- and 3-year endpoints included death, HF
hospitalization, stroke, TIA, and atrial flutter or AF recurrence.
RESULTS:
Age averaged 65.1 ± 10.7 years and 64.1% male. One- and 3-year endpoints of death, HF hospitalization, stroke, TIA, and atrial flutter or AF recurrence were statistically similar between manual and RMN treated groups. Fluoroscopy times were significantly lower in the RMN group compared to the manual ablation group (8.47 ± 0.45 vs. 9.63 ± 4.06 minutes, P < 0.0001). CF guided patients had 1-year recurrence rate of AF/atrial flutter statistically identical to patients treated with RMN (36.8% vs. 38.6%; P = 1.00).
CONCLUSION:
RMN results in outcomes similar to manual navigation. The addition of CF sensing catheters did not improve relative procedural outcome or safety profile in comparison to RMN guided ablation in this large observational study of AF ablation.
We encourage you to access the full publication online.
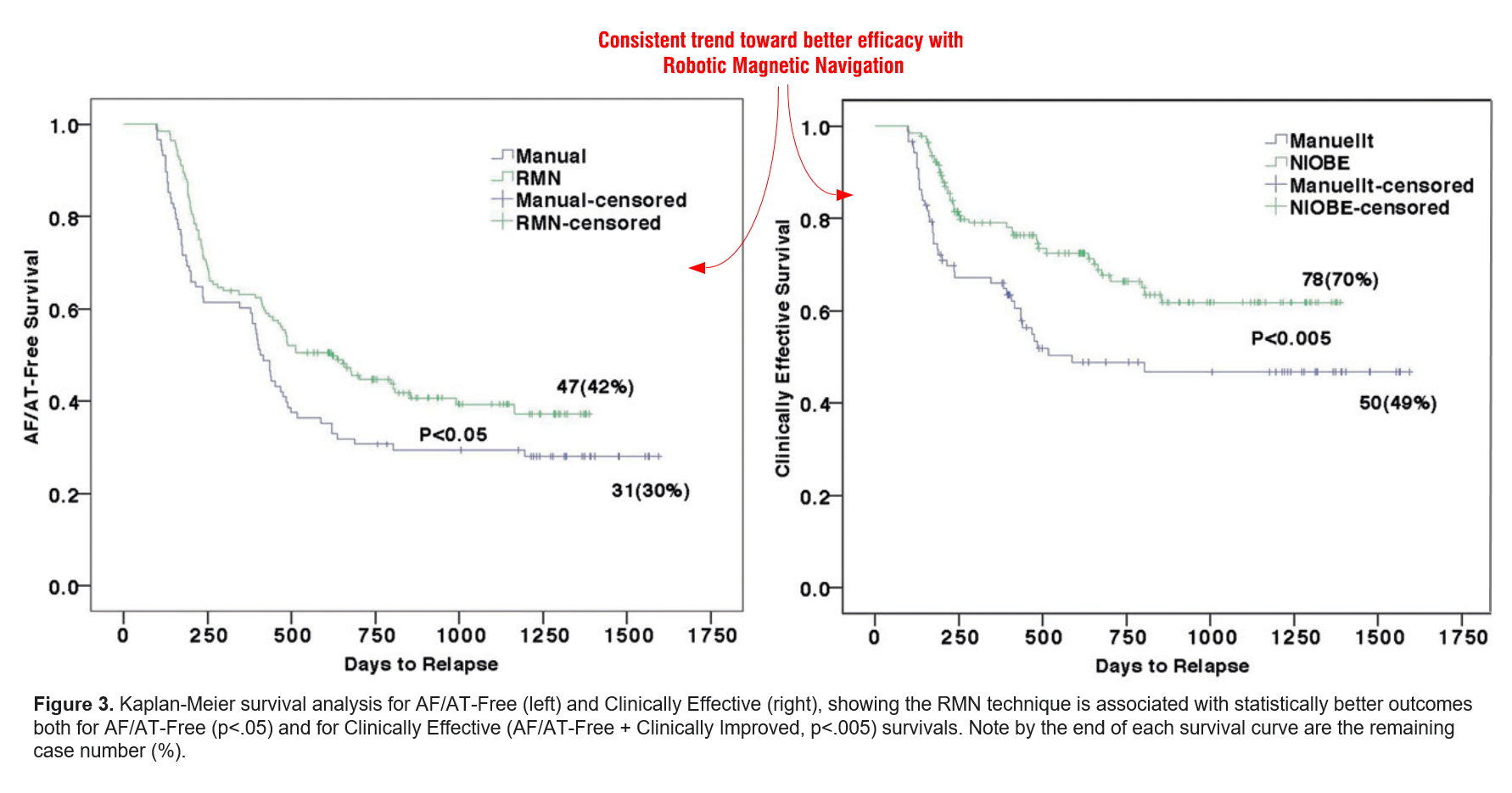
Long-term outcomes of the current remote magnetic catheter navigation technique for ablation of atrial fibrillation
Yuan S, Holmqvist F, Kongstad O, Jensen SM, Wang L, Ljungström E, Hertervig E, Borgquist R | Scandinavian Cardiovascular Journal. Vol 51, Issue 1, pp 308-315, December 2017
OBJECTIVES:
Comparisons between remote magnetic (RMN) and manual catheter navigation for atrial fibrillation (AF) ablation have earlier been reported with controversial results. However, these reports were based on earlier generations of the RMN system.
DESIGN:
To evaluate the outcomes of the most current RMN system for AF ablation in a larger patient population with longer follow-up time, 112 patients with AF (78 paroxysmal, 34 persistent) who underwent AF ablation utilizing RMN (RMN group) were compared to 102 AF ablation patients (72 paroxysmal, 30 persistent) utilizing manual technique (Manual group).
RESULTS:
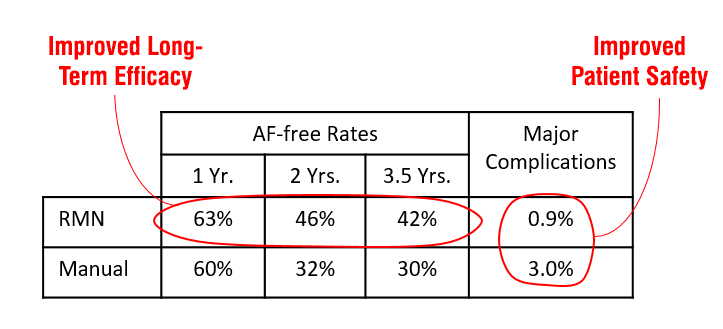
The RMN group was associated with significantly shorter fluoroscopy time (10.4 ± 6.4 vs. 16.3 ± 10.9 min, p<.001) but used more RF energy (64.1 ± 19.4KJ vs. 54.3 ± 24.1 KJ, p<.05), while total procedure time showed no significant difference (201 ± 35 vs. 196± 44 min, NS). After 39 ± 9/44 ± 10 months of follow-up, AF-free rates at 1year, 2 years and 3.5 years post ablation were 63%, 46% and 42% in the RMN group vs. 60%, 32% and 30% (survival analysis p<.05) in the Manual group, whereas clinically effective rates were 82%, 73% and 70% for the former vs. 70%, 56% and 49% for the latter (survival analysis p<.005).
CONCLUSION:
Differing from previous reports, our data from a larger patient population and longer follow-up time demonstrates that compared to manual technique, the most current RMN technique is associated with better procedural and clinical outcomes for AF ablation.
We encourage you to access the full publication online.
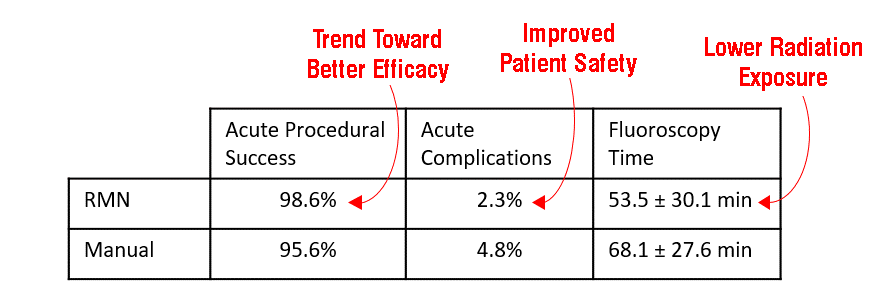
Remote magnetic catheter navigation versus conventional ablation in atrial fibrillation ablation: Fluoroscopy reduction
Lim PCY, Toh JJH, Loh JKXY, Lee ECY, Chong DTT, Tan BY, Ho KL, Ching CK, Teo WS | Journal of Arrhythmia. Vol 33, Issue 3, pp 167-171, June 2017
BACKGROUND:
Percutaneous transcatheter radiofrequency ablation of atrial fibrillation with remote controlled magnetic navigation (RMN) has been shown to reduce radiation exposure to patients and physicians compared with conventional manual (MAN) ablation techniques.
METHODS:
Catheter ablation for atrial fibrillation was performed utilizing RMN in 214 consecutive patients and MAN ablation techniques in 229 patients. We compared the fluoroscopy and procedural times between RMN and MAN catheter ablation of atrial fibrillation. Secondary objectives included comparing acute procedural success and short-term complication rates between both ablation strategies.
RESULTS:
Fluoroscopy time was significantly shorter in the RMN group than the MAN group (53.5 ± 30.1 vs 68.1 ± 27.6 min, respectively; p<0.01); however, the total procedural time was longer in the RMN group (280.2 ± 74.4 min vs 213.1 ± 64.75, respectively; p>0.001). Further subgroup analysis of the most recent 50 ablations each from the RMN and MAN groups, to attenuate the RMN learning curve effect, showed an even greater difference in fluoroscopy time (RMN vs MAN: 53.5 ± 30.1 vs 68.1 ± 27.6 min), though a consistently longer procedure time with RMN (249.5 ± 65.5 vs 186.3 ± 65.6 min, respectively). The acute procedural success rate was comparable between the groups (98.6% vs 95.6%, respectively; p=0.07). The rates of acute complications were similar in both groups (2.3% vs 4.8%, respectively; p=0.16).
CONCLUSIONS:
In radiofrequency ablation of atrial fibrillation, RMN appears to significantly reduce fluoroscopy time compared with conventional MAN ablation, though at a cost of increased total procedural time, with comparable acute success rates and safety profile. A reduction in procedure and fluoroscopy times is possible with gaining experience.
We encourage you to access the full publication online.
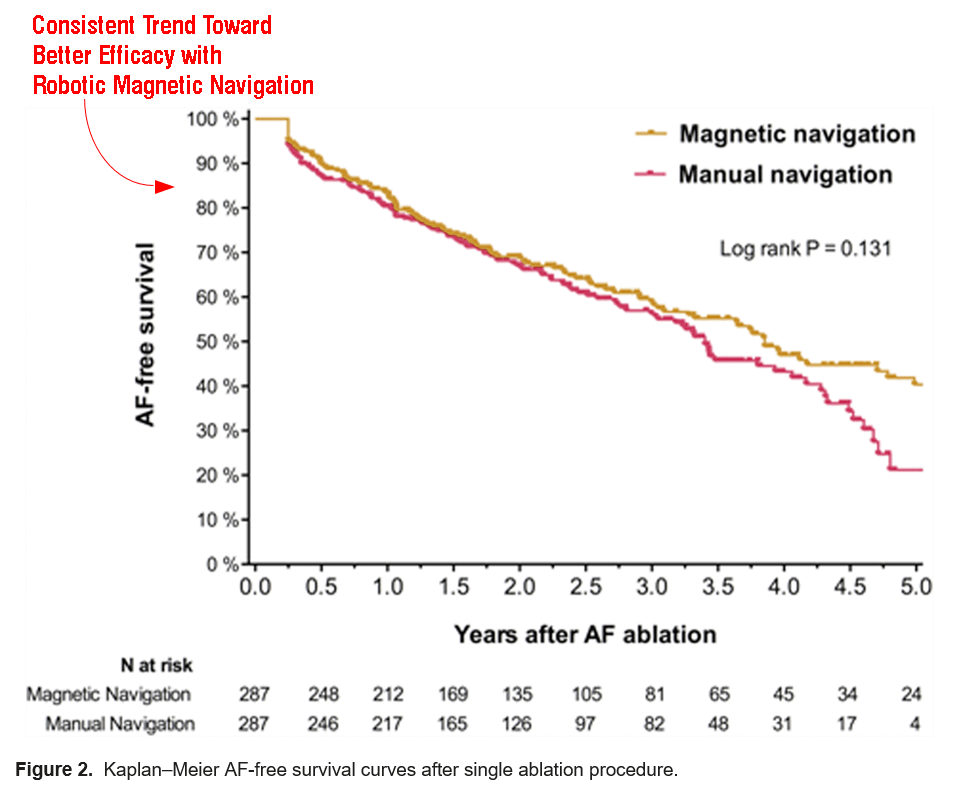
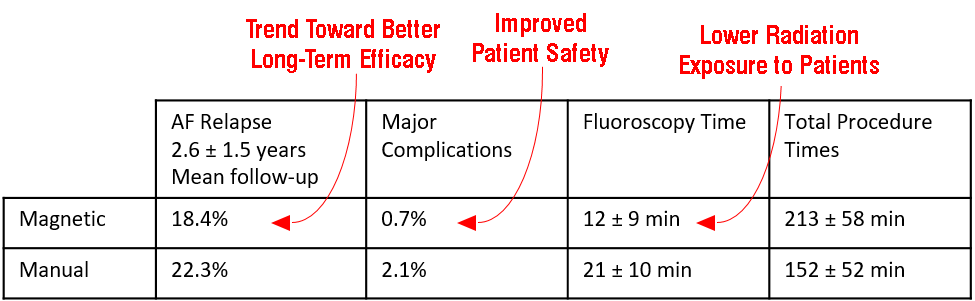
Safety and Long-Term Outcomes of Catheter Ablation of Atrial Fibrillation Using Magnetic Navigation versus Manual Conventional Ablation: A Propensity-Score Analysis
Adragão PP, Cavaco D, Ferreira AM, Costa FM, Parreira L, Carmo FM, Morgado FB, Santos KR, Santos PG, Carvalho MS, Durazzo A, Marques H, Gonҫalves PA, Raposo L, Mendes M | Journal of Cardiovascular Electrophysiology. Vol 27, Suppl 1, pp S11-S16, March 2016
INTRODUCTION:
Whether or not the potential advantages of using a magnetic navigation system (MNS) translate into improved outcomes in patients undergoing atrial fibrillation (AF) ablation is a question that remains unanswered.
METHODS AND RESULTS:
In this observational registry study, we used propensity-score matching to compare the outcomes of patients with symptomatic drug-refractory AF who underwent catheter ablation using MNS with the outcomes of those who underwent catheter ablation using conventional manual navigation. Among 1,035 eligible patients, 287 patients in each group had similar propensity scores and were included in the analysis. The primary efficacy outcome was the rate of AF relapse after a 3-month blanking period. At a mean follow-up of 2.6 ± 1.5 years, AF ablation with MNS was associated with a similar risk of AF relapse as compared with manual navigation (18.4% per year and 22.3% per year, respectively; hazard ratio 0.81, 95% CI 0.63-1.05; P = 0.108). Major complications occurred in two patients (0.7%) using MNS, and in six patients (2.1%) undergoing manually navigated ablation (P = 0.286). Fluoroscopy times were 21 ± 10 minutes in the manual navigation group, and 12 ± 9 minutes in the MNS group (P = 0.001), whereas total procedure times were 152 ± 52 minutes and 213 ± 58 minutes, respectively (P = 0.001).
CONCLUSIONS:
In this propensity-score matched comparison, magnetic navigation and conventional manual AF ablations seem to have similar relapse rates and a similar risk of complications. AF ablations with magnetic navigation take longer to perform but expose patients to significantly shorter fluoroscopy times.
We encourage you to access the full publication online.
Efficacy and Safety of Atrial Fibrillation Ablation Using Remote Magnetic Navigation: Experience from 1,006 Procedures
Jin QI, Pehrson S, Jacobsen PK, Chen XU | Journal of Cardiovascular Electrophysiology. Vol 27, Suppl 1, pp S23-S28, March 2016
BACKGROUND:
The objective of this study was to assess the procedural outcomes of catheter ablation guided by remote magnetic navigation (RMN) in a large cohort of patients with paroxysmal atrial fibrillation (PAF) and persistent AF (PerAF).
METHODS:
A total of 726 patients (547 male, age: 58.5 ± 10.3 years) with symptomatic AF (61% PAF) were analyzed from a prospective ablation registry. Procedural parameters including pulmonary venous (PV) anatomy, left atrial (LA) volume, procedural time, ablation time, fluoroscopy time, total X-ray dose, and complications were assessed.
RESULTS:
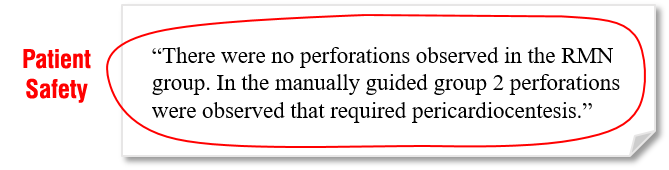
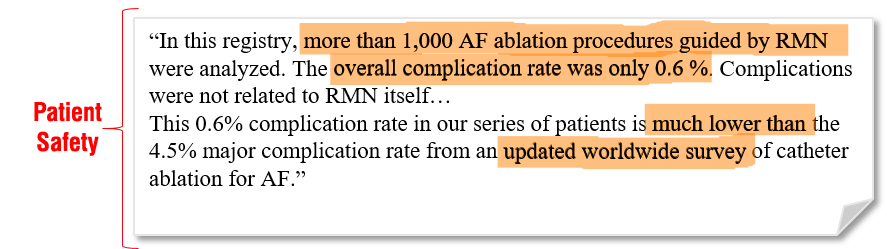
One thousand and six ablation procedures were analyzed. One-third of the patients (240/726) were ablated on more than one occasion, resulting in a mean of 1.3 ± 0.6 times for the entire group. When analyzing all procedures, the mean procedural time and ablation time was 134 ± 35 minutes and 2,130 ± 1,025 seconds, respectively. The mean fluoroscopy time was 5.4 ± 3.7 minutes. Compared to PAF patients, procedural time and ablation time were significantly increased in patients with PerAF by 10% (P < 0.001) and 19% (P < 0.001), respectively. However, fluoroscopy time was not increased (5.3 ± 3.5 minutes, PAF vs. 5.6 ± 4.0 minutes, PerAF, P = 0.17). The overall complication rate was 0.6%. One PAF patient experienced cardiac tamponade. AF repeat ablations by RMN significantly reduced the procedural and ablation times when compared with their first ablation times.
CONCLUSIONS:
AF ablation guided by RMN is safe as evidenced by a low complication rate. Fluoroscopy time was relatively short for both PAF and PerAF ablation.
We encourage you to view the full publication online.
The magnetic navigation system allows safety and high efficacy for ablation of arrhythmias
Bauernfeind T, Akca F, Schwagten B, de Groot N, Van Belle Y, Valk S, Ujvari B, Jordaens L, Szili-Torok T | EP Europace. Vol 13, Issue 7, pp 1015-1021, July 2011
AIMS:
We aimed to evaluate the safety and long-term efficacy of the magnetic navigation system (MNS) in a large number of patients. The MNS has the potential for improving safety and efficacy based on atraumatic catheter design and superior navigation capabilities.
METHODS & RESULTS:
In this study, 610 consecutive patients underwent ablation. Patients were divided into two age- and sex-matched groups. Ablations were performed either using MNS (group MNS, 292) or conventional manual ablation [group manual navigation (MAN), 318]. The following parameters were analysed: acute success rate, fluoroscopy time, procedure time, complications [major: pericardial tamponade, permanent atrioventricular (AV) block, major bleeding, and death; minor: minor bleeding and temporary AV block]. Recurrence rate was assessed during follow-up (15 ± 9.5 months). Subgroup analysis was performed for the following groups: atrial fibrillation, isthmus dependent and atypical atrial flutter, atrial tachycardia, AV nodal re-entrant tachycardia, circus movement tachycardia, and ventricular tachycardia (VT). Magnetic navigation system was associated with less major complications (0.34 vs. 3.2%, P = 0.01). The total numbers of complications were lower in group MNS (4.5 vs. 10%, P = 0.005). Magnetic navigation system was equally effective as MAN in acute success rate for overall groups (92 vs. 94%, P = ns). Magnetic navigation system was more successful for VTs (93 vs. 72%, P < 0.05). Less fluoroscopy was used in group MNS (30 ± 20 vs. 35 ± 25 min, P < 0.01). There were no differences in procedure times and recurrence rates for the overall groups (168 ± 67 vs. 159 ± 75 min, P = ns; 14 vs. 11%, P = ns; respectively).
CONCLUSIONS:
Our data suggest that the use of MNS improves safety without compromising efficiency of ablations. Magnetic navigation system is more effective than manual ablation for VTs.
 We encourage you to access the full publication online.
We encourage you to access the full publication online.
A meta-analysis of manual versus remote magnetic navigation for ventricular tachycardia ablation
Turagam MK, Atkins D, Tung R, Mansour M, Ruskin J, Cheng J, Di Biase L, Natale A, Lakkireddy D | Journal of Interventional Cardiac Electrophysiology. Vol 49, Issue 3, pp 227-235, September 2017
BACKGROUND:
There are limited studies on the safety and efficacy of remote magnetic navigation (RMN) versus manual navigation (MAN) in ventricular tachycardia (VT) ablation.
METHODS:
A comprehensive literature search was performed using the keywords VT ablation, stereotaxis, RMN and MAN in Pubmed, Ebsco, Web of Science, Cochrane, and Google scholar databases.
RESULTS:
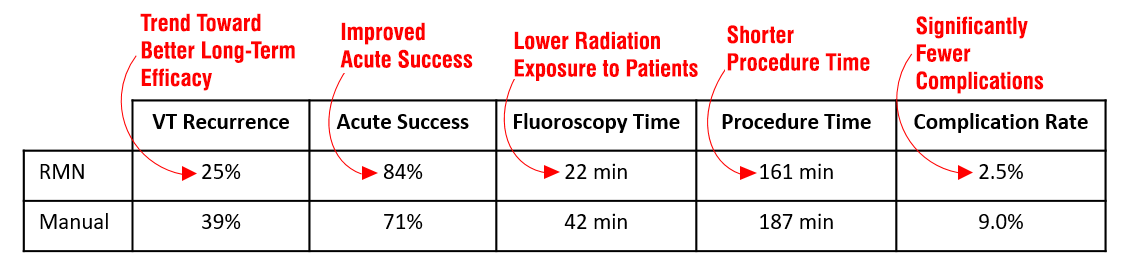
The analysis included seven studies (one randomized, three prospective observational, and three retrospective) including 779 patients [both structural heart disease (SHD) and idiopathic VT] comparing RMN (N = 433) and MAN (N = 339) in VT ablation. The primary end point of long-term VT recurrence was significantly lower with RMN (OR 0.61, 95% CI 0.44–0.85, p = 0.003) compared with MAN. Other end points of acute procedural success (OR 2.13, 95% CI 1.40–3.23, p = 0.0004) was significantly higher with RMN compared with MAN. Fluoroscopy [mean difference −10.42, 95% CI −12.7 to −8.1, p < 0.0001], procedural time [mean difference −9.79, 95% CI −19.27 to −0.3, p = 0.04] and complications (OR 0.35, 95% CI 0.17–0.74, p = 0.0006) were also significantly lower in RMN when compared with MAN. In a subgroup analysis SHD, there was no significant difference in VT recurrence or acute procedural success with RMN vs. MAN. In idiopathic VT, RMN significantly increased acute procedural success with no difference in VT recurrence.
CONCLUSIONS:
The results demonstrate that RMN is safe and effective when compared with MAN in patients with both SHD and idiopathic VT undergoing catheter ablation. Further prospective studies are needed to further verify the safety and efficacy of RMN.
 We encourage you to access the full publication online.
We encourage you to access the full publication online.
Comparison of remote magnetic navigation ablation and manual ablation of idiopathic ventricular arrhythmia after failed manual ablation
Kawamura M, Scheinman MM, Tseng ZH, Lee BK, Marcus GM, Badhwar N | Journal of Interventional Cardiac Electrophysiology. Vol 48, Issue 1, pp 35-42, January 2017
PURPOSE:
Catheter ablation for idiopathic ventricular arrhythmia (VA) is effective and safe, but efficacy is frequently limited due to an epicardial origin and difficult anatomy. The remote magnetic navigation (RMN) catheter has a flexible catheter design allowing access to difficult anatomy. We describe the efficacy of the RMN for ablation of idiopathic VA after failed manual ablation.
METHODS:
Among 235 patients with idiopathic VA referred for catheter ablation, we identified 51 patients who were referred for repeat ablation after a failed manual ablation. We analyzed the clinical characteristics, including the successful ablation site and findings at electrophysiology study, in repeat procedures conducted using RMN as compared with manual ablation. Among these patients, 22 (43 %) underwent repeat ablation with the RMN and 29 (57 %) underwent repeat ablation with a manual ablation.
RESULTS:
Overall, successful ablation rate was significantly higher using RMN as compared with manual ablation (91 vs. 69 %, P = 0.02). Fluoroscopy time in the RMN was 17 ± 12 min as compared with 43 ± 18 min in the manual ablation (P = 0.009). Successful ablation rate in the posterior right ventricular outflow tract (RVOT) plus posterior-tricuspid annulus was higher with RMN as compared with manual ablation (92 vs. 50 %, P = 0.03). Neither groups exhibited any major complications.
CONCLUSIONS:
The RMN is more effective in selected patients with recurrent idiopathic VA after failed manual ablation and is associated with less fluoroscopy time. The RMN catheters have a flexible design enabling them to access otherwise difficult anatomy including the posterior tricuspid annulus and posterior RVOT.
We encourage you to access the full publication online.
Catheter Ablation of Ventricular Tachycardias Using Remote Magnetic Navigation: A Consecutive Case–Control Study
Szili-Torok T, Schwagten B, Akca F, Bauernfeind T, Abkenari LD, Haitsma D, Van Belle Y, Groot ND, Jordaens L | Journal of Cardiovascular Electrophysiology. Vol 23, Issue 9, pp 948-954, September 2012
BACKGROUND:
This study aimed to compare acute and late outcomes of VT ablation using the magnetic navigation system (MNS) to manual techniques (MAN) in patients with (SHD) and without (NSHD) structural heart disease.
METHODS:
Ablation data of 113 consecutive patients (43 SHD, 70 NSHD) with ventricular tachycardia treated with catheter ablation at our center were analyzed. Success rate, complications, procedure, fluoroscopy, and ablation times, and recurrence rates were systematically recorded for all patients.
RESULTS:
A total of 72 patients were included in the MNS group and 41 patients were included in the MAN group. Patient age, gender, and right ventricular and left ventricular VT were equally distributed. Acute success was achieved in 59 patients in the MNS group (82%) versus 27 (66%) patients in the MAN group (P = 0.046). Overall procedural time (177 ± 79 vs 232 ± 99 minutes, P < 0.01) and mean patient fluoroscopy time (27 ± 19 vs 56 ± 32 minutes, P < 0.001) were all significantly lower using MNS. In NSHD pts, higher acute success was achieved with MNS (83,7% vs 61.9%, P = 0.049), with shorter procedure times (151 ± 57 vs 210 ± 96, P = 0.011), whereas in SHD‐VT these were not significantly different. No major complications occurred in the MNS group (0%) versus 1 cardiac tamponade and 1 significantly damaged ICD lead in the MAN group (4.9%, NS). After follow‐up (20 ± 11 vs 20 ± 10 months, NS), VT recurred in 14 pts (23.7%) in the MNS group versus 12 pts (44.4%) in the MAN group (P = 0.047).
CONCLUSIONS:
The use of MNS offers advantages for ablation of NSHD-VT, while it offers similar efficacy for SHD-VT. (J Cardiovasc Electrophysiol, Vol. 23, pp. 948-954, September 2012).
We encourage you to access the full publication online.
Remote magnetic navigation shows superior long-term outcomes in pediatric atrioventricular (nodal) tachycardia ablation compared to manual radiofrequency and cryoablation
Noten A, Kammeraad J, Misier N, Wijchers S, van Beynum I, Dalinghaus M, Krasemann T, Yap S, de Groot N, Szili-Torok T,| International Journal of Cardiology Heart and Vascular. Vol 37, October 2021
Background
Catheter ablation (CA) is the first-choice treatment for tachyarrhythmia in children. Currently available CA techniques differ in mechanism of catheter navigation and energy sources. There are no large studies comparing long-term outcomes between available CA techniques in a pediatric population with atrioventricular reentry tachycardia (AVRT) or atrioventricular nodal reentry tachycardia (AVNRT) mechanisms.
Methods
This single-center, retrospective study included all first consecutive CA procedures for AVRT or AVNRT performed in children without structural heart disease from 2008 to 2019. Three study groups were defined by the ablation technique used: RMN, MAN or CRYO. Primary outcome was long-term recurrence of tachyarrhythmia.
Results
In total, we included 223 patients, aged 14 (IQR 12–16) years; weighting 56 (IQR 47–65) kilograms. In total, 108 procedures were performed using RMN, 76 using MAN and 39 using CRYO. RMN had significantly lower recurrence rates compared to MAN and CRYO at mean follow-up of 5.5 ± 2.9 years (AVRT: 4.3% versus 15.6% versus 54.5%, P < 0.001; AVNRT: 7.7% versus 8.3% versus 35.7%, P = 0.008; for RMN versus MAN versus
CRYO respectively). In AVNRT ablation, RMN had significantly lower fluoroscopy doses compared to CRYO [30 (IQR 20–41) versus 45 (IQR 29–65) mGy, P = 0.040).
Conclusions
In pediatric patients without structural heart disease who underwent their first AV(N)RT ablation, RMN has superior long-term outcomes compared to MAN and CRYO, in addition to favorable fluoroscopy doses.
We encourage you to access the full publication online.
Remote Magnetic Navigation for Catheter Ablation in Patients with Congenital Heart Disease: A Review
Roy K, Gomez-Pulido F, Ernst S | Journal of Cardiovascular Electrophysiology. Vol 27, Issue S1, pp S45-S56, March 2016
Review on Remote Magnetic Navigation in Congenital Heart Disease
In patients with congenital heart disease, challenges to catheter‐based arrhythmia interventions are unique and numerous given the complexity of the underlying defects, anatomic and surgical intervention variants including baffles, conduits, patches, and/or shunts. Remote magnetic navigation offers significant advantages in these cases that may present with limited vascular access or difficult access to the target cardiac chambers implicated by the previous surgical interventions. We reviewed the data available on the safety, feasibility, and effectiveness of magnetic navigation for the treatment of arrhythmia in congenital heart disease and discussed the specific challenges related to various congenital defects and repair with the potential advantages offered by magnetic navigation in these circumstances.
We encourage you to access the full publication online.
Contemporary Outcomes of Supraventricular Tachycardia Ablation in Congenital Heart Disease: A Single-Center Experience in 116 Patients
Ueda A, Suman-Horduna I, Mantziari L, Gujic M, Marchese P, Ho SY, Babu-Narayan SV, Ernst S | Circulation: Arrhythmia and Electrophysiology. Vol 6, Issue 3, June 2013
BACKGROUND:
Remote magnetic navigation–guided ablation with 3-dimensional (3D)-image integration could provide maximum benefit in patients with complex anatomy. We reviewed supraventricular tachycardia (SVT) ablation in adult patients with congenital heart disease to assess the contribution of these technologies.
METHODS & RESULTS:
One hundred fifty-four SVT ablation procedures (228 SVTs) using a 3D-electroanatomic mapping system in 116 adult patients with congenital heart disease (mean age, 41; 76 male) were classified into 3 groups: Group A, manual mapping/ablation (n=60 procedures); Group B, remote magnetic navigation–guided mapping/ablation with normal femoral vein access (49); and Group C, remote magnetic navigation–guided mapping/ablation with difficult access (45). Group A included simple anomalies with less SVTs. Group B comprised predominantly Fontan patients with more SVTs. Group C included more complex defects, such as intra-atrial baffle or interrupted inferior venous access, in which retrograde aortic and superior venous accesses were used exclusively with more frequent use of image integration (97.8%; P<0.001). Acute success was 91.5%, 83.7%, and 82.2%, respectively (P=0.370). In group C, fluoroscopy time was the shortest (median, 4.2 min; P<0.001) despite the longer procedure duration (median, 253 min; P<0.001). SVTs free rates were 80.4%, 82.4%, and 75.8%, respectively (P=0.787) during a mean 20-months follow-up period.
CONCLUSIONS:
The combination of remote magnetic navigation, 3D-image integration, and electroanatomic mapping system facilitated safe and feasible ablation with very low fluoroscopy exposure even in patients with complex anomalies.
 We encourage you to access the full publication online.
We encourage you to access the full publication online.
Publications Database
We welcome you to investigate further. Click to view a searchable database of all publications referencing Stereotaxis.
- Szili-Torok T, Schwagten B, Akca F, Bauernfeind T, Abkenari LD, Haitsma D, et al. Catheter ablation of ventricular tachycardias using remote magnetic navigation: a consecutive case-control study. J Cardiovasc Electrophysiol. 2012;23(9):948-54.
- Kim JJ, Macicek SL, Decker JA, Kertesz NJ, Friedman RA, Cannon BC. Magnetic versus manual catheter navigation for ablation of free wall accessory pathways in children. Circ Arrhythm Electrophysiol. 2012; 2012;5:804-8.
- Dinov B, Schönbauer R, Wojdyla-Hordynska A, Braunschweig F, Richter S, Altmann D, et al. Long-term efficacy of single procedure remote magnetic catheter navigation for ablation of ischemic ventricular tachycardia: a retrospective study. J Cardiovasc Electrophysiol. 2012;23(5):499-505.
- Roudijk RW, Gujic M, Suman-Horduna I. Catheter ablation in children and young adults: is there an additional benefit from remote magnetic navigation? Net Heart J. 2013;21:296–303.
- Akca F, Theuns DAMJ, Dabiri Abkenari L, de Groot NMS, Jordaens L, Szili-Torok T. Outcomes of repeat catheter ablation using magnetic navigation or conventional ablation. EP Europace. 2013;15(10):1426-31.
- Koutalas E, Bertagnolli L, Sommer P, Richter S, Rolf S, Breithardt O, et al. Efficacy and safety of remote magnetic catheter navigation vs. manual steerable sheath-guided ablation for catheter ablation of atrial fibrillation: a case-control study. Europace. 2015;17(2):232-8.
- Hendriks AA, Akca F, Dabiri Abkenari L, Khan M, Bhaqwandien R, Yap SC, et al. Safety and clinical outcome of catheter ablation of ventricular arrhythmias using contact force sensing: consecutive case series. J Cardiovasc Electrophysiol. 2015;26(11):1224-9.
- Akca F, Janse P, Theuns DA, and Szili-Torok T. A prospective study on safety of catheter ablation procedures: contact force guided ablation could reduce the risk of cardiac perforation. Int J Cardiol. 2015;179:441-8.
- Di Biase L, Tung R, Burkhardt JD, Romero J, Trivedi C, Mohanty S, et al. Scar homogeneization ablation in patients with ischemic cardiomyopathy: comparison between remote magnetic navigation and manual ablation. Circulation. 2015;132 Suppl 3.
- Weiss JP, May HT, Bair TL, Crandall BG, Cutler MJ, Day JD, et al. A Comparison of Remote Magnetic Irrigated Tip Ablation versus Manual Catheter Irrigated Tip Catheter Ablation With and Without Force Sensing Feedback. J Cardiovasc Electrophysiol. 2016;27 Suppl 1:S5-S10.
- Adragão PP, Cavaco D, Ferreira AM, Costa FM, Parreira L, Carmo P, et al. Safety and Long-Term Outcomes of Catheter Ablation of Atrial Fibrillation Using Magnetic Navigation versus Manual Conventional Ablation: A Propensity-Score Analysis. J Cardiovasc Electrophysiol. 2016;27 Suppl 1:S11-6.
- Kawamura M, Scheinman MM, Tseng ZH, Lee BK, Marcus GM, Badhwar N. Comparison of remote magnetic navigation ablation and manual ablation of idiopathic ventricular arrhythmia after failed manual ablation. J Interv Card Electrophysiol. 2017;48(1):35-42.
- Reents T, Jilek C, Schuster P, Nölker G, Koch-Büttner K, Ammar-Busch S, et al. Multicenter, randomized comparison between magnetically navigated and manually guided radiofrequency ablation of atrioventricular nodal reentrant tachycardia (the MagMa-AVNRT-trial). Clin Res Cardiol. 2017;106(12):947-52.
- Lim PCY, Toh JJH, Loh J, Lee ECY, Chong DTT, Tan BY, et al. Remote magnetic catheter navigation versus conventional ablation in atrial fibrillation ablation: Fluoroscopy reduction. J Arrhythm. 2017;33(3):167-71.
- Yuan S, Holmqvist F, Kongstad O, Jensen SM, Wang L, Ljungström E, et al. Long-term outcomes of the current remote magnetic catheter navigation technique for ablation of atrial fibrillation. Scand Cardiovasc J. 2017;51(6):308-15.
- Kataria V, Berte B, Vandekerckhove Y, Tavernier R, and Duytschaever M. Remote Magnetic versus Manual Navigation for Radiofrequency Ablation of Paroxysmal Atrial Fibrillation: Long-Term, Controlled Data in a Large Cohort. Biomed Res Int. 2017;2017:6323729.
- Qiu X, Zhang N, Luo Q, Liu A, Ji Y, Ye J, et al. Remote magnetic navigation facilitates the ablations of frequent ventricular premature complexes originating from the outflow tract and the valve annulus as compared to manual control navigation. Int J Cardiol. 2018;267:94-99.
- Bollmann A, Ueberham L, Schuler E, Wiedemann M, Reithmann C, Sause A, et al. Cardiac tamponade in catheter ablation of atrial fibrillation: German-wide analysis of 21 141 procedures in the Helios atrial fibrillation ablation registry (SAFER). EP Europace. 2018.
- Katsiyiannis WT, Melby DP, Matelski JL, Ervin VL, Laverence KL, and Gornick CC. Feasibility and safety of remote-controlled magnetic navigation for ablation of atrial fibrillation. Am J Cardiol. 2008;102(12):1674-6.
- Miyazaki S, Shah AJ, Xhaet O, Derval N, Matsuo S, Wright M, et al. Remote magnetic navigation with irrigated tip catheter for ablation of paroxysmal atrial fibrillation. Circ Arrhythm Electrophysiol. 2010;3(6):585-9.
- Sorgente A, Chierchia GB, Capulzini L, Yazaki Y, Muller-Burri A, Bayrak F, et al. Atrial fibrillation ablation: a single center comparison between remote magnetic navigation, cryoballoon and conventional manual pulmonary vein isolation. Indian pacing and electrophysiology journal. 2010;10(11):486.
- Arya A, Zaker-Shahrak R, Sommer P, Bollmann A, Wetzel U, Gaspar T, et al. Catheter ablation of atrial fibrillation using remote magnetic catheter navigation: a case-control study. Europace. 2011;13(1):45-50.
- Choi MS, Oh YS, Jang SW, Kim JH, Shin WS, Youn HJ, et al. Comparison of magnetic navigation system and conventional method in catheter ablation of atrial fibrillation: is magnetic navigation system is more effective and safer than conventional method? Korean Circ J. 2011;41(5):248-52.
- Luthje L, Vollmann D, Seegers J, Dorenkamp M, Sohns C, Hasenfuss G, et al. Remote magnetic versus manual catheter navigation for circumferential pulmonary vein ablation in patients with atrial fibrillation. Clin Res Cardiol. 2011;100(11):1003-11.
- Solheim E, Off MK, Hoff PI, De Bortoli A, Schuster P, Ohm OJ, et al. Remote magnetic versus manual catheters: evaluation of ablation effect in atrial fibrillation by myocardial marker levels. J Interv Card Electrophysiol. 2011;32(1):37-43.
- Pappone C, Vicedomini G, Manguso F, Gugliotta F, Mazzone P, Gulletta S, et al. Robotic magnetic navigation for atrial fibrillation ablation. J Am Coll Cardiol. 2006;47(7):1390-400.
- Di Biase L, Fahmy TS, Patel D, Bai R, Civello K, Wazni OM, et al. Remote Magnetic Navigation: Human Experience in Pulmonary Vein Ablation. Journal of the American College of Cardiology. 2007;50(9):868-74.
- Augello G, Vicedomini G, Saviano M, Crisa S, Mazzone P, Ornago O, et al. Pulmonary vein isolation after circumferential pulmonary vein ablation: comparison between Lasso and three-dimensional electroanatomical assessment of complete electrical disconnection. Heart Rhythm. 2009;6(12):1706-13.
- Chun KR, Wissner E, Koektuerk B, Konstantinidou M, Schmidt B, Zerm T, et al. Remote-controlled magnetic pulmonary vein isolation using a new irrigated-tip catheter in patients with atrial fibrillation. Circ Arrhythm Electrophysiol. 2010;3(5):458-64.
- Pappone C, Vicedomini G, Frigoli E, Giannelli L, Ciaccio C, Baldi M, et al. Irrigated-tip magnetic catheter ablation of AF: a long-term prospective study in 130 patients. Heart Rhythm. 2011;8(1):8-15.
- Muntean B, Gutleben KJ, Heintze J, Vogt J, Horstkotte D, and Nolker G. Magnetically guided irrigated gold-tip catheter ablation of persistent atrial fibrillation–techniques, procedural parameters and outcome. J Interv Card Electrophysiol. 2012;35(2):163-71.
- Nolker G, Gutleben KJ, Muntean B, Vogt J, Horstkotte D, Dabiri Abkenari L, et al. Novel robotic catheter manipulation system integrated with remote magnetic navigation for fully remote ablation of atrial tachyarrhythmias: a two-centre evaluation. Europace. 2012;14(12):1715-8.
- Da Costa A, Ben H’Dech M, Romeyer-Bouchard C, Bisch L, Gate-Martinet A, Levallois M, et al. Remote-controlled magnetic pulmonary vein isolation using a new three-dimensional non-fluoroscopic navigation system: A single-centre prospective study. Archives of Cardiovascular Diseases. 2013;106(8):423-32.
- Sohns C, Sohns JM, Bergau L, Sossalla S, Vollmann D, Luthje L, et al. Pulmonary vein anatomy predicts freedom from atrial fibrillation using remote magnetic navigation for circumferential pulmonary vein ablation. Europace. 2013;15(8):1136-42.
- Bun SS, Latcu DG, and Saoudi N. Remote magnetic ablation of atrial fibrillation is safe and feasible in the presence of a left atrial appendage closure device. Europace. 2014;16(4):476.
- de Vries LJ, Akca F, Khan M, Dabiri-Abkenari L, Janse P, Theuns DAMJ, et al. Clinical outcome of ablation for long-standing persistent atrial fibrillation with or without defragmentation. Netherlands Heart Journal. 2014;22(1):30-6.
- Gate-Martinet A, Da Costa A, Romeyer-Bouchard C, Bisch L, Levallois M, and Isaaz K. Does a patent foramen ovale matter when using a remote-controlled magnetic system for pulmonary vein isolation? Arch Cardiovasc Dis. 2014;107(2):88-95.
- Pezawas T, Ristl R, Bilinski M, Schukro C, and Schmidinger H. Single, remote-magnetic catheter approach for pulmonary vein isolation in patients with paroxysmal and non-paroxysmal atrial fibrillation. Int J Cardiol. 2014;174(1):18-24.
- Sohns C, Bergau L, Seegers J, Luthje L, Vollmann D, and Zabel M. Single-ring ablation compared with standard circumferential pulmonary vein isolation using remote magnetic catheter navigation. J Interv Card Electrophysiol. 2014;41(1):75-82.
- Vollmann D, Luthje L, Seegers J, Sohns C, Sossalla S, Sohns J, et al. Remote magnetic navigation for circumferential pulmonary vein ablation: single-catheter technique or additional use of a circular mapping catheter? J Interv Card Electrophysiol. 2014;41(1):65-73.
- Da Costa A, Levallois M, Romeyer-Bouchard C, Bisch L, Gate-Martinet A, and Isaaz K. Remote-controlled magnetic pulmonary vein isolation combined with superior vena cava isolation for paroxysmal atrial fibrillation: a prospective randomized study. Arch Cardiovasc Dis. 2015;108(3):163-71.
- Errahmouni A, Latcu DG, Bun SS, Rijo N, Dugourd C, and Saoudi N. Remotely controlled steerable sheath improves result and procedural parameters of atrial fibrillation ablation with magnetic navigation. Europace. 2015;17(7):1045-50.
- Jin Q, Pehrson S, Jacobsen PK, and Chen X. Impact of catheter ablation with remote magnetic navigation on procedural outcomes in patients with persistent and long-standing persistent atrial fibrillation. J Interv Card Electrophysiol. 2015;44(2):197-204.
- Hugle B, Buchter, B. Doneva, Z., Geissler, A., Sell, L., Tso, T. Mirazchiyski, S., Sha, Q. Combined Use of a High-Density Multi-electrode Mapping Catheter and a Magnetically Navigated Ablation Catheter for Atrial Fibrillation Procedures: A Feasibility Study. The Journal Of Innovations in Cardiac Rythm Management. 2016;7:2413-7.
- Jin QI, Pehrson S, Jacobsen PK, and Chen XU. Efficacy and Safety of Atrial Fibrillation Ablation Using Remote Magnetic Navigation: Experience from 1,006 Procedures. J Cardiovasc Electrophysiol. 2016;27 Suppl 1:S23-8.
- Nolker G, Schwagten B, Deville JB, Burkhardt JD, Horton RP, Sha Q, et al. Vdrive Evaluation of Remote Steering and Testing in Lasso Electrophysiology Procedures Study: The VERSATILE Study in Atrial Fibrillation Ablation. J Cardiovasc Electrophysiol. 2016;27 Suppl 1:S17-22.
- Lin C, Pehrson S, Jacobsen PK, and Chen X. Initial experience of a novel mapping system combined with remote magnetic navigation in the catheter ablation of atrial fibrillation. J Cardiovasc Electrophysiol. 2017;28(12):1387-92.
- Maurer T, Sohns C, Deiss S, Rottner L, Wohlmuth P, Reißmann B, et al. Significant reduction in procedure duration in remote magnetic-guided catheter ablation of atrial fibrillation using the third-generation magnetic navigation system. Journal of Interventional Cardiac Electrophysiology. 2017;49(3):219-26.
- Yagishita A, Gimbel J, OLIVEIRA S, Manyam H, Sparano D, Cakulev I, et al. Long‐Term Outcome of Left Atrial Voltage‐Guided Substrate Ablation During Atrial Fibrillation: A Novel Adjunctive Ablation Strategy. Journal of cardiovascular electrophysiology. 2017;28(2):147-55
- Data on file.
Stereotaxis Intended Use Statements, United States Labeling:
The Genesis RMN® and Niobe® ES Systems are intended to navigate compatible magnetic devices through tissue to designated target sites in the right and left heart, coronary vasculature, neurovasculature, and peripheral vasculature by orienting the device tip in a desired direction. The Cardiodrive® Catheter Advancement System (CAS) is intended to automatically advance and retract compatible magnetic electrophysiology (EP) mapping and ablation catheters inside a patient’s heart when used in conjunction with a Stereotaxis magnetic navigation system. The Cardiodrive System is not intended to advance the EP mapping and ablation catheters through the coronary vasculature or the coronary sinus.
Consult the associated product labeling for the Indications for Use and instructions of other devices used in conjunction with Stereotaxis products.
Cardiodrive and Niobe are trademarks of Stereotaxis, Inc., registered in the United States, the European Community, and Japan. Genesis RMN is a trademark of Stereotaxis, Inc., registered in the United States.